Obstructed Defaecation
Link To New Dedicated Obstructed Defaecation Website
What is obstructed defaecation?
This means difficulty in emptying the rectum even in the presence of soft motions. It may also be associated with constipation (infrequent or hard motions). The differentiation is important, as the causes are different and management is also different. Both constipation and obstructed defaecation may co-exist
| |
Constipation |
Obstructed defaecation |
| Definition |
Infrequent defaecation, less than once every 3 days or passing very hard stools or both |
Difficulty in evacuation or emptying the rectum. This may occur even with frequent visits to the toilet and even with passing soft motions |
| Associated conditions |
Simple constipation, slow transit constipation |
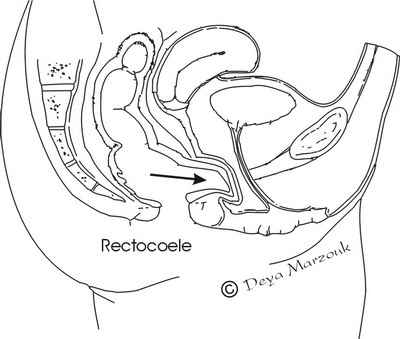
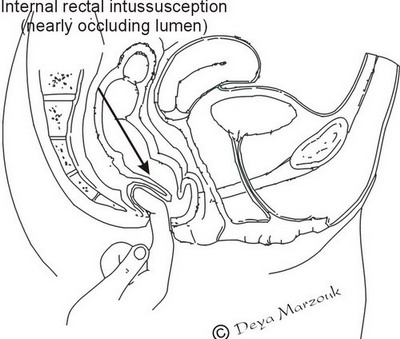
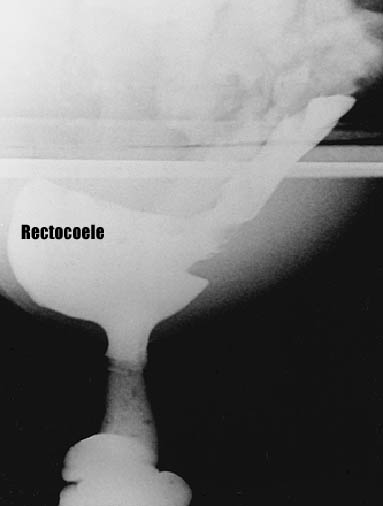
Internal rectal intussusception, rectocoele, anismus |
| |
|
|
Warning!
It is vital that other more serious colorectal diseases are excluded first before assuming that a patient is suffering from obstructed defaecation. For example sigmoid & rectal cancer may masquerade as obstructed defaecation (although there is usually associated bleeding & mucous discharge). This is usually straightforward and may be accomplished by examination with sigmoidoscopy. Patients with short term symptoms (less than 1 year) should probably undergo a colonoscopy or a barium enema to exclude other colorectal diseases before diagnosing functional problems such as obstructed defaecation or constipation.
Symptoms
Patients often complain of severe difficulty in evacuation, prolonged straining, feeling of incomplete evacuation and needing to go again shortly after finishing the first attempt at defaecation. Patients may be unable to evacuate without either pressure on the perineum or supporting the back wall of the vagina. Some resort to using fingers inside the rectum to extract faeces. Patients also report discomfort in the perineum, feeling that they are sitting on an egg or something falling down.
Examination
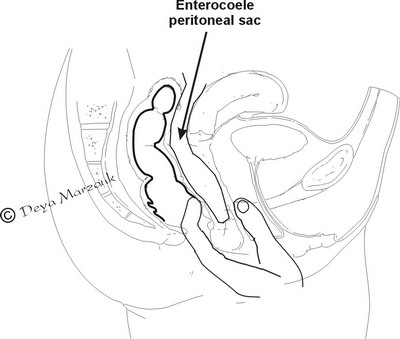
Standard abdominal and rectal examination (and sometimes vaginal examination) is carried out. This may reveal perineal descent, presence of badder prolapse (cystocoele), uterine prolapse, rectocoele, internal rectal intussusception, enterocoele or a combination of these abnormalities. Rarely, some patients may exhibit inability to relax the anal sphincters on attempted defaection (anismus)
Investigations
Although in the majority of patients the diagnosis is clear to an expert in this field, it is desirable to get anorectal physiology testing done. This is essential in patients with severe symptoms and those in whom surgery is contemplated. It allows (among other things) for assessment of the presence of associated slow transit constipation, the contribution of any rectocoele or intussusception to the difficulty or incompletness of evacuation and their respective importance in the defaecation disorder.
Treatment
Treatment should be conservative at first. The majority of patients will improve with education about the dynamics of their disordered defaecation and hence the importance of avoiding straining particularly when there is a significant intussusception. Some patients with large rectocoele may find that supporting the posterior vaginal wall is acceptable during defaecation. Many would not like it as a long term solution, but the success of this suggest that surgical repair of rectocoele may be successful. All patients benefit from eating more vegetables & fruit (unless they have loose motions). Many would find that using glycerine suppositories is a better help than laxatives (which helps constipation, but may not be helpful in this situation). Biofeedback may help. The help of community advice nurse is invaluable.
Surgery is indicated in those who fail initial conservative treatment and is directed towards the likely cause (i.e. the rectocoele or the internal rectal intussusception or both). This is further disccussed in the relevant web pages